
Out-Of-Hospital CPAP vs BiPAP
On a clear, crisp fall morning, you and your partner are called to the home of a 78-year-old male patient with trouble breathing.
As you enter the home, you see a male patient in obvious respiratory distress. His respiratory rate is near 30 breaths per minute and his oxygen saturation is around 80% on room air. He has a history of both COPD and CHF. He states the difficulty breathing started last night and has become progressively worse throughout the morning. On auscultation, you hear both diffuse wheezing and bilateral wheezing. His heart rate is 130 and his blood pressure is 180/98.
He appears anxious and is profusely diaphoretic. He denies chest pain or any allergies to medications. His prescription medications include an albuterol inhaler, Symbicort, nitroglycerin, metoprolol, and amlodipine. He has a history of myocardial infarction, hypertension, and states he has never been intubated for his COPD. He has a 40 pack-per-year history of smoking but states he quit after his heart attack.
You quickly place the patient on CPAP and start transport to your local emergency department. En route to the hospital, you obtain a 12 lead ECG, IV access, and start a nebulized treatment of albuterol and ipratropium. His oxygen saturation improves to 90%. You add continuous waveform capnography and continue to monitor vital signs. Once the hospital report is given, the patient is successfully transferred over to BiPAP.
Over the course of your career, you notice that the emergency department does one of a couple of things: They either transfer the patient to BiPAP, intubate the patient with an endotracheal tube, or remove CPAP but continue to monitor the patient’s respiratory status. You wonder why CPAP is not continued in hospital and wonder what the big difference is between the two.
Ventilation and Oxygenation
To begin, let us first explain how normal ventilation and oxygenation works. Ventilation is the physical movement of air into and out of the lungs. Oxygenation is the actual gas exchange between oxygen and carbon dioxide at a cellular level.
Normal ventilation occurs when the diaphragm contracts and negative pressure pulls the lungs down and open. The pressure difference from the atmosphere and the gases inside the lungs creates airflow. The thoracic wall resembles a bucket handle. Each rib is a bucket handle, and as they move up and laterally, the vertical diameter increases.
This is different than mechanical ventilation or the use of positive pressure ventilation, which uses positive pressure to open the lungs and force air, specifically oxygen, into the lungs. Both BiPAP and CPAP use negative and positive pressure to force oxygen into the lungs. Both can be uncomfortable for the body since normal ventilation is usually passive and requires negative pressure.
Ventilation occurs with air movement into and out of the lung regardless of negative pressure or positive pressure. Oxygenation requires the actual exchange of gases at an alveolar or cellular level. When oxygenation occurs, oxygen is drawn in and crosses the alveoli of the lungs and into the bloodstream. Then carbon dioxide leaves the bloodstream and is released into the environment during exhalation.
Prior to the use of CPAP or BiPAP, EMS providers had to use bag-valve masks to provide manual ventilation and then endotracheal intubation for deteriorating patients. Manual bag-mask ventilation led to more barotrauma from too high of pressure and could cause a pneumothorax or volutrauma that stretchers the alveoli and decreases the overall elasticity of the alveoli and causes inflammation and decreases the ability for gas exchange.
When using CPAP or BiPAP, oxygenation occurs by delivering oxygenated air, usually at high concentrations, directly to the lungs and prevents alveolar collapse, therefore allowing more alveolar recruitment. Oxygen can move from the lungs and into the bloodstream via the capillaries of the alveoli. Carbon dioxide is then exchanged for oxygen. During exhalation, the carbon dioxide is released, and the intercostal muscles relax, decreasing the vertical diameter.
CPAP
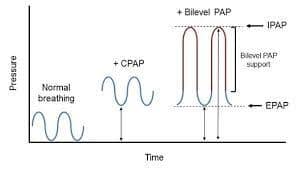
CPAP uses positive-end expiratory pressure, also known as PEEP. A person’s normal PEEP when breathing on their own is usually between 3-5 cmH2O. In the EMS setting, CPAP can deliver oxygenated air at levels of 5, 7, and 10 cmH2o. The pressure remains constant, so when the patient needs to exhale, they must do so against the PEEP that CPAP creates. This is difficult for many patients; however, it may be necessary to open the alveoli and allow oxygenation to occur. The patient must maintain spontaneous respirations for the use of either CPAP or BiPAP.
CPAP masks come in different varieties or systems. Masks can cover over the nose and mouth, the nose only, the mouth only, or at the base of the nostrils. There are 3 main components of a typical CPAP mask. They consist of a mask frame, a mask headgear, a mask cushion, and a flow generator. The frame allows the mask to be secured by the headgear. The cushion is provided for patient comfort and to create an airtight seal. In the EMS setting, almost all CPAP devices utilize the full-face mask system.
The CPAP mask PEEP is either controlled by a PEEP valve or by adjusting the flow of oxygen delivered to provide a Venturi type effect, where both room air and high-flow oxygen are forced through a narrow opening, creating PEEP at different levels.
BiPAP
BiPAP is more comfortable because it senses the pressure differences during inhalation and exhalation. PEEP on inhalation may be 10cmH20 and exhalation may be 5cmH20, as an example. The pressure difference allows the patient to feel more comfortable and makes the act of breathing easier.
The inspiratory positive airway pressure is known as IPAP and the expiratory positive airway pressure is known as EPAP. BiPAP provides more control of the respiratory cycle and is generally easier to optimize cardiopulmonary performance. Both inhalation and exhalation PEEP can be fine-tuned to the comfort of the patient as symptoms either improve or decompensate further. Worsening of symptoms will generally lead to endotracheal intubation and the patient being placed on a ventilator. Improvement will generally lead to the patient coming off CPAP or BiPAP to a non-rebreather mask or nasal cannula.
CPAP vs. BiPAP
 While CPAP is available to almost every pre-hospital provider, BiPAP is not. CPAP only requires an oxygen regulator and an airtight mask that comes with a strap system to secure the mask to the face and head. The mask must be tight-fitting and not allow for air leaks in order to maintain the pressure or PEEP. Many CPAP systems also allow for a nebulized treatment to be delivered at the same time.
While CPAP is available to almost every pre-hospital provider, BiPAP is not. CPAP only requires an oxygen regulator and an airtight mask that comes with a strap system to secure the mask to the face and head. The mask must be tight-fitting and not allow for air leaks in order to maintain the pressure or PEEP. Many CPAP systems also allow for a nebulized treatment to be delivered at the same time.
The nebulized bronchodilators help decrease lung tissue inflammation and help open the bronchioles and alveoli. PEEP is achieved by changing the flow amount of oxygen delivered to the mask or by using a PEEP valve that is attached to the CPAP mask system. Patients with COPD generally need a PEEP of 5cmH2o versus the CHF patient who will require higher amounts of PEEP, around 10cmH2O. Delivering CPAP at those levels can reduce the work of breathing and increase oxygenation. The downside of using CPAP is that it tends to take longer for the patient to improve work of breathing and, as stated before, is more uncomfortable for the patient.
BiPAP will require a similar closed unit mask system but will also require a machine or ventilator to control the different levels of PEEP. Hospitals prefer better control and patients generally are much more comfortable using BiPAP as it mimics the normal respiratory pressure differences. Studies have shown a decrease in mortality with patients who received BiPAP and a decrease in the need for intubation. Only critical care paramedics are usually capable of delivering BiPAP in the field. The critical care provider would not only carry the airtight mask but also a ventilator. BiPAP will also require a prescribed respiratory rate, which will determine the time frame of both inhalation and exhalation time. Fraction of inspired oxygen, also known as FiO2, can be titrated as the patient has improving respiratory status.
Both CPAP and BiPAP are considered noninvasive forms of positive pressure ventilation. CPAP in most EMS systems is considered a standing order that even some basic EMTs are utilizing in many states. It does require more training than an EMT will receive in their basic EMT course, but with the right training and understanding of the disease processes, EMT basics have been quite successful and advanced providers, such as paramedics, have been able to stay in service for higher acuity calls. CPAP is utilized in most EMS systems due to the simplicity of the procedure.
BiPAP would be more expensive and require much more training and, in many systems, would require a critical care paramedic level or higher. EMS providers must be prepared to “coach” their patients and explain the process. The masks can make the patient feel claustrophobic, which will make many patients “fight” the process and increase their work of breathing. When the patient tolerates the mask and the increase PEEP, the work of breathing should decrease, and their respiratory status should improve. Providers may want to start with simply holding the mask to the patient’s face until they feel a bit more comfortable before securing the headgear straps. Lastly, the advanced care provider can consider a low dose of benzodiazepine to help provide some sedation and lower feelings of anxiety.
Waveform Capnography
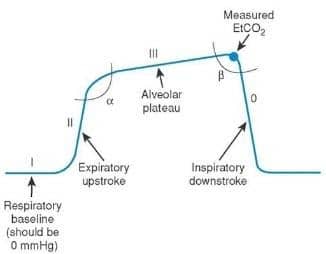 Patients utilizing positive pressure ventilation with either CPAP or BiPAP should have continuous waveform capnography monitoring. The normal ETCO2 waveform has 4 phases, and they should have a square box-shaped appearance.
Patients utilizing positive pressure ventilation with either CPAP or BiPAP should have continuous waveform capnography monitoring. The normal ETCO2 waveform has 4 phases, and they should have a square box-shaped appearance.
Phase 1 is the exhalation of the dead-space air that does not contain carbon dioxide. This air did not reach the alveoli. Phase 1 ends when air with carbon dioxide begins to be detected and will sharply increase then will plateau at the highest level of carbon dioxide.
Phase 2 is the sharp rise of detected carbon dioxide.
Stage 3 should be an even level as the person fully exhales, and once the total lung volume of air is released, phase 3 will end as carbon dioxide levels begin to drop once again.
Stage 4 will show the quick fall back to atmospheric air that no longer has enough carbon dioxide to register on waveform capnography.
The ETCO2 is a noninvasive technique that will measure the amount of exhaled carbon dioxide. Normal values of ETCO2 readings should be between 35-45 mmHg. Exhaled carbon dioxide reflects the patient’s cardiac output and oxygenation. Both metabolic function and respiratory function can be assessed and changes in PEEP or amount of oxygen can be adjusted to continue support of the patient’s respiratory status.
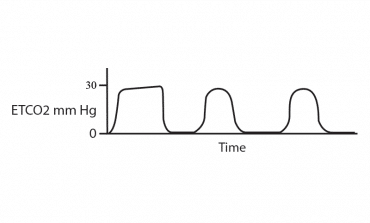
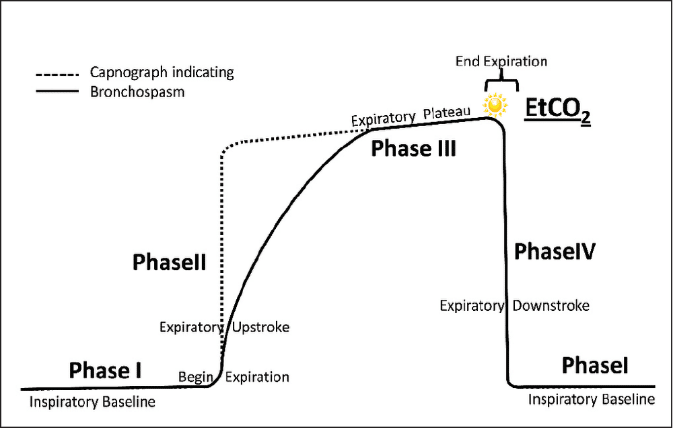 Initial ETCO2 waveform on a COPD patient will likely have a shark fin type waveform. The plateau of the ETCO2 in the patient experiencing bronchoconstriction will be very short and the upscale will not be as dramatic as the normal patient’s waveform. By evaluating the COPD patient’s ETCO2 waveform, the EMS professional can determine the amount of airflow restriction and can decide if the severity requires CPAP or BiPAP. Once either is utilized, the EMS professional can use the ETCO2 waveform to evaluate the effectiveness of the CPAP or BiPAP treatment.
Initial ETCO2 waveform on a COPD patient will likely have a shark fin type waveform. The plateau of the ETCO2 in the patient experiencing bronchoconstriction will be very short and the upscale will not be as dramatic as the normal patient’s waveform. By evaluating the COPD patient’s ETCO2 waveform, the EMS professional can determine the amount of airflow restriction and can decide if the severity requires CPAP or BiPAP. Once either is utilized, the EMS professional can use the ETCO2 waveform to evaluate the effectiveness of the CPAP or BiPAP treatment.
With COPD, many times nebulized bronchodilators will be used in conjunction with the CPAP or BiPAP mask to help the bronchioles open and allow the positive pressure airflow to reach deeper into the lungs so the oxygen can reach the alveoli. The ETCO2 reading tends to be higher in a COPD patient. Remember that these patients may initially feel very uncomfortable and may even panic once the mask is placed on their face, especially when utilizing CPAP due to the higher-than-normal pressure being delivered. The patient may feel like they cannot breathe out against the pressure, which is why BiPAP tends to be tolerated better by patients and why hospitals tend to switch patients to BiPAP who arrive on CPAP with the EMS crew.
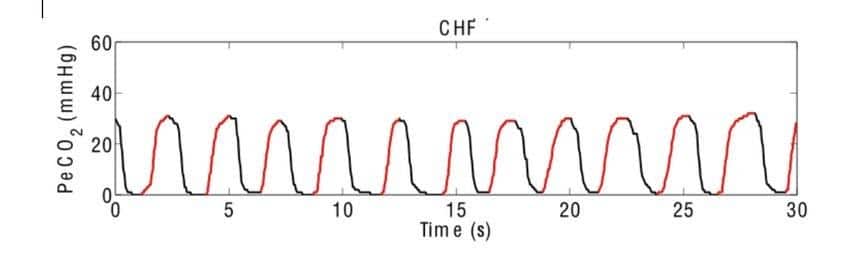 The patient experiencing a CHF exacerbation will have a quicker waveform with a very short plateau and lower than normal ETCo2. The lungs in this disease will likely become filled with fluid, known as pulmonary edema, which decreases the number of alveoli available for gas exchange. ETCO2 readings will be lower than 35mmHg. The lung sounds of a CHF patient will usually present with rale or crackles in the lungs. The higher the sounds of rales in the lung field directly correlates with the amount of fluid in the lungs. Oxygen can go in but, without gas exchange at the alveoli, carbon dioxide will not be exchanged for oxygen, which results in lower ETCO2.
The patient experiencing a CHF exacerbation will have a quicker waveform with a very short plateau and lower than normal ETCo2. The lungs in this disease will likely become filled with fluid, known as pulmonary edema, which decreases the number of alveoli available for gas exchange. ETCO2 readings will be lower than 35mmHg. The lung sounds of a CHF patient will usually present with rale or crackles in the lungs. The higher the sounds of rales in the lung field directly correlates with the amount of fluid in the lungs. Oxygen can go in but, without gas exchange at the alveoli, carbon dioxide will not be exchanged for oxygen, which results in lower ETCO2.
Initially, the patient’s body compensates for the lower amount of oxygen by increasing their respiratory rate, thus “blowing off more carbon dioxide.” When a patient with CHF has both high blood pressure and high ETCO2, the EMS professional should consider the patient to be in respiratory failure. It is at this point where the increased respiratory rate and accessory muscle use begin to fail. The body will now start to have shallow breathing and retention of carbon dioxide leading to higher ETCO2 readings. The ETCO2 readings will now be above 45mmHg. CPAP and BiPAP are utilized in this patient to force the fluid out of the lungs and allow for more alveolar recruitment and increasing oxygenation.
 If CPAP or BiPAP is not initiated quickly enough or if the patient also presents with cardiogenic shock, the patient will now have low ETCO2 readings, below 35mmHg, which is an indication of poor tissue perfusion. The waveform will become rounded and resemble tombstones.
If CPAP or BiPAP is not initiated quickly enough or if the patient also presents with cardiogenic shock, the patient will now have low ETCO2 readings, below 35mmHg, which is an indication of poor tissue perfusion. The waveform will become rounded and resemble tombstones.
Both CPAP and BiPAP, when utilized on the severe COPD and CHF patient, can lower the need for endotracheal intubation. The results of CPAP should take effect quickly. A rise in ETCO2 would suggest the patient is now breathing deeper and cardiopulmonary function is improving. The goal would be to be able to obtain normal ETCO2 numbers by the time the EMS crew arrives at the hospital. If, however, the EMS professional is not able to maintain perfusion and oxygenation, the EMS professional will need to reassess the situation and consider rapid sequence intubation for complete respiratory failure.
Contraindications and Complications
There are some contraindications of applying CPAP or BiPAP to a patient experiencing a COPD or CHF exacerbation. These include:
- If the patient has an altered level of consciousness and cannot protect their airway
- Cardiogenic shock that requires pressor support
- Uncontrolled bleeding in the gastrointestinal tract
- Facial trauma where creating a good mask seal would be compromised
- Facial burns also would prevent creating a tight seal
- External masses or upper airway obstruction and tracheal injuries that would not allow the pressurized airflow to adequately flow to the alveoli
Any of these contraindications could lead to the airflow being forced out of the respiratory tract and into the surrounding tissues and spaces.
As well as contraindications, CPAP and BiPAP can have complications. Besides patient discomfort, the EMS professional should be cognizant of barotrauma, specifically pneumothorax. Hypotension can occur if there is too much intrathoracic pressure causing a decrease in cardiac output. Air escaping into the abdominal cavity can lead to abdominal compartment syndrome. Care should also be used to monitor for subcutaneous emphysema or air leaking into the neck under the skin that becomes trapped. If the EMS provider remembers to pay close attention to the patient’s respiratory status, the risks of complications can be greatly reduced.
Other Indications for CPAP and BiPAP
Besides COPD and CHF, there are several other indications for the use of CPAP or BiPAP. Toxic inhalation injuries that cause pulmonary edema. When the hazardous agent is inhaled by the patient, the lung tissue becomes damaged and is irritated and inflamed. The use of CPAP or BiPAP can help alleviate pulmonary edema. Smoke inhalation can also cause bronchospasm or narrowing of airways. With CPAP or BiPAP, the patient will be less likely to have intrapulmonary shunting. In carbon monoxide poisoning, the use of non-invasive positive pressure can be used to mimic the hyperbaric chamber that is normally used to push the carbon monoxide off the hemoglobin. Those patients should receive 100% oxygen regardless whether CPAP or BiPAP is used.
Conditions that cause pulmonary edemata like saltwater drowning, high-altitude pulmonary edema, and organophosphate poisoning can benefit from positive pressure ventilation to help push the fluid out internally and reopen the alveoli allowing for better alveolar recruitment. Improving atelectasis is the main goal with using CPAP and BiPAP for freshwater drowning, community-acquired pneumonia, and flail chest. Care must be taken by the EMS provider to not provide too much pressure and cause barotrauma, but successful delivery of positive end pressure ventilation has been shown to decrease mortality rate in these types of patients. All of these conditions could also have BiPAP utilized, however, the setting and adjusting of pressures for each specific patient usually requires more education, which is often why EMS will only provide CPAP and leave BiPAP for in-hospital treatment.
With the resounding improvement of the use of positive pressure ventilation in the EMS setting, patients suffering from acute respiratory failure have been treated and managed successfully in the pre-hospital setting, and patient morbidity and mortality have decreased. By understanding the fundamentals of the respiratory system and how non-invasive positive pressure ventilation works, the EMS provider can start treatment in the field and transportation can occur to a higher level of care where treatment can be continued without major delay to patient treatment.
References:
- CPAP The Push For Rapid Relief. https://aironusa.com/wp-content/uploads/2017/10/JEMS-CPAP-2011-full1.pdf
- Volutrama and Atelectrauma: Which Is Worse? https://ccforum.biomedcentral.com/articles/10.1186/s13054-018-2199-2
- BiPAP Unwrapped: How Non-Invasive Ventilation Helps Patients in Respiratory Failure. https://www.jems.com/2008/01/31/bipap-unwrapped-how-non-invasi/
- Evidence-Based EMS: Out-of-Hospital BiPAP vs. CPAP. https://www.emsworld.com/article/12145134/evidence-based-ems-out-of-hospital-bipap-vs-cpap
- Airway Management: BiPAP vs. CPAP. https://www.ems1.com/ems-products/medical-equipment/airway-management/articles/airway-management-bi-pap-vs-cpap-1yDNcTghlyfxo0zO/
- EMS, Prehospital CPAP Devices. https://www.ncbi.nlm.nih.gov/books/NBK470429/
 Kuo Downing-Reese is a 16-year veteran of EMS. She started her career in Los Angeles County in a variety of settings, including private ambulance, fire, and hospital ED. Kuo went to paramedic school at UCLA-Daniel Freeman. She has a degree in EMS management from George Washington University and currently practices as a full-time critical care paramedic in Rochester, New York. She also does a variety of EMS and medical training as a NYS Certified Lab Instructor (CIC intern), NAEMT instructor, and as AHA regional/training center faculty.
Kuo Downing-Reese is a 16-year veteran of EMS. She started her career in Los Angeles County in a variety of settings, including private ambulance, fire, and hospital ED. Kuo went to paramedic school at UCLA-Daniel Freeman. She has a degree in EMS management from George Washington University and currently practices as a full-time critical care paramedic in Rochester, New York. She also does a variety of EMS and medical training as a NYS Certified Lab Instructor (CIC intern), NAEMT instructor, and as AHA regional/training center faculty.


